Rethinking Evidence in Hemophilia Care: A Critical Analysis of International Consensus Guidelines
Cedric Hermans, MD, PhD, FRCP(Lon, Edin)
Full Professor, Head Haemostasis and Thrombosis Unit
Haemophilia Clinic Division of Adult Haematology St-Luc University Hospital (Brussels), Vice-President Medical of the WFH
Continuing our editorial series featuring insights from leading experts participating in GARDEN ECM webinars, this contribution brings scientific discussion from our educational activities to the broader hematology community.
Prof. C. Hermans critically examines current international hemophilia guidelines and the role of evidence in shaping clinical practice.
Introduction
Haemophilia is a rare inherited bleeding disorder caused by a deficiency of clotting factor VIII or IX, leading to regular bleeding episodes, particularly within joints and muscles, and progressive joint damage over time (Chowdary et al., 2025; Gualtierotti et al., 2021). Although it is not very widespread, hemophilia has a significant clinical burden because of its chronicity, heterogeneity of clinical manifestation, and long-term complications that impair physical functioning and quality of life (Benemei et al., 2024).
The therapeutic environment of hemophilia has been changing fast over the last 10 years, with the release of the extended half-life factor concentrates, no-factor treatment like emicizumab, and the advent of gene therapy as a potential curative approach (Carcao et al., 2024; Samelson-Jones et al., 2024). These developments have transformed the image of care and made it more reactive to the treatment of bleeding and more proactive to the treatment that emphasizes the long-term consequences (Srivastava et al., 2020).
Clinical practice guidelines have taken center stage in this highly complicated therapeutic setting that offers systematic recommendations aimed at standardization of care and better patient outcomes across the world (Rezende et al., 2024). Nevertheless, the development of such guidelines in rare diseases is always a challenging task. The generation and interpretation of evidence are complicated by limited patient populations, lack of high-quality comparative trials, and the fast changing treatment options (Iorio et al., 2023). Consequently, various organizations might use various methodological frameworks, resulting in the diversity of recommendations and, in certain instances, contradictory advice (Lewandowska et al., 2025).
This has been discussed in a recent webinar organized by Cedric Hermans that discussed the international consensus recommendations regarding the management of hemophilia and the implications of varying evidence frameworks. Specifically, the difference between the broad and globally focused recommendations of the World Federation of Hemophilia and the more limited and evidence-focused approach of the International Society on Thrombosis and Hemostasis is a matter of concern concerning the role of evidence, the trade-off between methodological rigor and practical relevance, and the overall effect of guidelines on care access and therapeutic development (Rezende et al., 2024).
Evolution and Role of Hemophilia Guidelines
The history of hemophilia management guidelines has been dynamic and changing over the last twenty years; it is both an increase in clinical evidence as well as a growth in the complexity of care. The initial attempts, including the initial draft of the guidelines released by the World Federation of Hemophilia in 2005, were mostly subjective and based on the informal consensus, with scanty literature review.
These first principles were significant in the creation of a basis of standardized care, specifically in an environment where specialized expertise was scarcely available. Nevertheless, their methodological shortcomings were also indicative of the larger issues of evidence generation in rare diseases where comparative trials of high quality were limited (Srivastava et al., 2020).
Later versions indicate a definite transition to more organized and rigorous methods. In 2012, systematic literature reviews were included in the second edition of the WFH guidelines and the first aspects of evidence grading were introduced, signifying a shift towards more formalized evidence-based practice.
The third edition in 2020 has seen the creation of numerous more guidelines, with large international teams of experts, systematic methodologies such as Delphi consensus processes, and massive syntheses of available evidence in many different areas of care (Srivastava et al., 2020). This evolution highlights an increasing concern with methodological clarity, multidisciplinary input, and generalizability, the most recent guidelines (2020) featuring over 300 practice recommendations regarding different fields of hemophilia care. In addition to their methodological development, the role of hemophilia guidelines has increased. Modern guidelines no longer serve to offer clinical guidance to specific practitioners; they serve as an important tool in the development of healthcare policy, resource distribution, and quality of care in various health systems (Rezende et al., 2024).
Their prevalence and use in clinical and academic settings highlight their impact on shaping best practice across the globe. Notably, in low- and middle-income contexts, these guidelines can become major reference points to develop the treatment frameworks where local expertise or infrastructure is not available (Fedewa et al., 2025).
Nevertheless, more methodological sophistication does not always translate to enhanced clinical relevance. The proliferation of therapeutic modalities, such as extended half-life factor concentrates, non-factor therapies, and gene therapy has exceeded the capacity of conventional evidence hierarchies to record actual-world effectiveness and patient-centered results (Carcao et al., 2024; Samelson-Jones et al., 2024).
Such a tension can be seen especially when comparing various guideline frameworks. Although other organizations have embraced more inclusive methods including those of the WFH, which incorporates clinical knowledge and real-life evidence, other organizations have focused on having higher levels of evidence. This difference brings up some key questions about the purpose of guidelines in rare diseases: are they supposed to reflect the best available evidence, or are they supposed to be practical, accommodating variation in practice and resource availability (Iorio et al., 2023; Lewandowska et al., 2025).
Structure and Scope of Contemporary Hemophilia Guidelines (WFH vs ISTH)
The growing complexity of hemophilia treatment has resulted in the creation of many international guideline frameworks, the most prominent of which are those published by the World Federation of Hemophilia and the International Society on Thrombosis and Hemostasis. Although the two seek to enhance patient outcomes by using standardized recommendations, their structure, scope, and methodological philosophies vary significantly, with significant clinical practice implications.
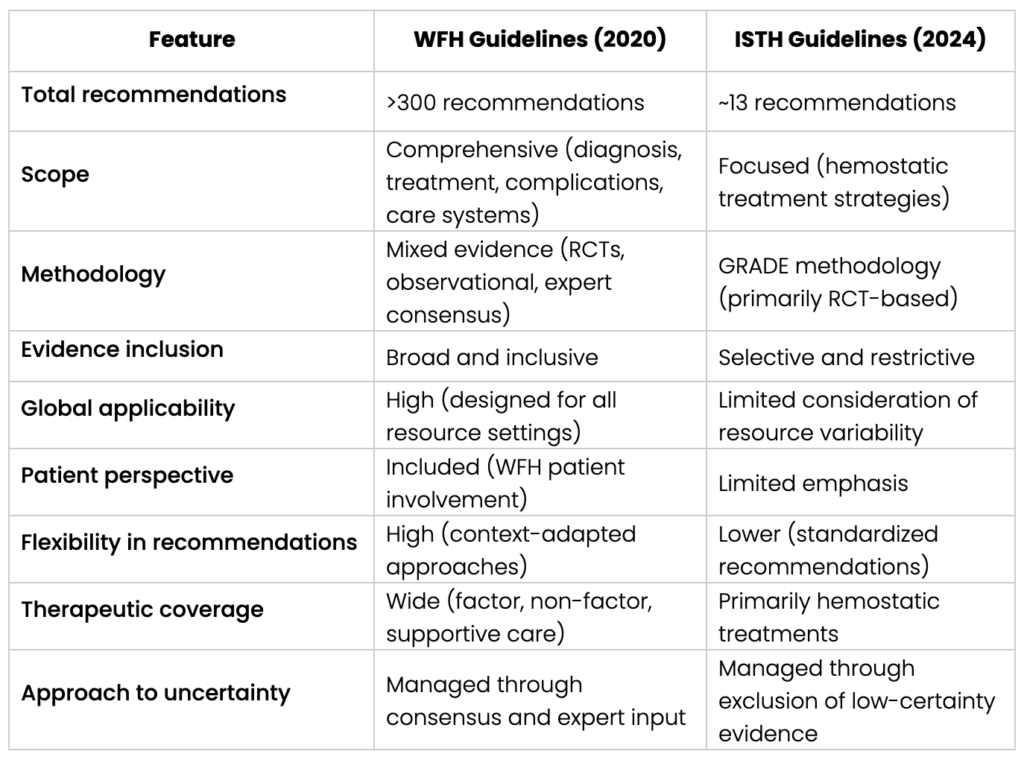
One of the most extensive global guidelines that can be found is the WFH Guidelines on the Management of Hemophilia (3rd edition, 2020) which covers more than 300 individual recommendations and a broad scope of clinical areas, such as diagnosis, prophylaxis, inhibitor management, complications, and comprehensive care provision (Srivastava et al., 2020). These guidelines have been made globally applicable and are clearly meant to consider variability in healthcare infrastructure, resource availability, and patient populations.
In this regard, they combine a wide scope of evidence sources, such as observational studies, registry data, expert opinion, and patient views, along with randomized controlled trials (RCTs). By contrast, the ISTH 2024 clinical practice guideline is more focused and methodologically restrictive. The ISTH guideline is developed based on the GRADE framework and focuses on the high-certainty evidence obtained mainly through RCTs and has a narrow scope to the major hemostatic treatment options in hemophilia A and B (Rezende et al., 2024). This leads to a succinct list of about 13 main recommendations, based on issues like prophylaxis versus episodic therapy, factor versus non-factor therapy, and treatment in certain clinical situations, as they have been reflected in the webinar.
The expanded WFH guidelines allow clinicians to address complicated, real-life situations, such as access variability to therapies and patient differences. As an illustration, the consideration of lower-dose prophylaxis approaches and alternative treatment options is an indication of the awareness of the limitations in low- and middle-income nations, where the best treatment options are not always available (Srivastava et al., 2020; Fedewa et al., 2025).
Key Comparison Between WFH (2020) and ISTH (2024) Guidelines
Methodological Divide – Randomized Controlled Trials versus Real-World Evidence
One of the main problems of the modern development of hemophilia guidelines is the methodological gap between the use of randomized controlled trials (RCTs) and the incorporation of real-world evidence. This difference, which is emphasized in the webinar, is the basis of the core dissimilarity between the suggestions of the International Society on Thrombosis and Hemostasis and the World Federation of Hemophilia.
The ISTH guideline uses a rigid hierarchy of evidence based on the GRADE methodology, with high-certainty evidence that is mainly based on RCT (Rezende et al., 2024). Such a strategy aligns with the principles of evidence-based medicine, in which RCTs are regarded as the gold standard because of their capacity to reduce bias and determine causation. Nevertheless, RCTs have good internal validity but their use in rare diseases like hemophilia is also constrained by nature. The limited patient populations, high inclusion criteria, and limited follow-up time tend to create evidence that is not representative of the complexity of the clinical practice in the real world (Iorio et al., 2023).
Conversely, the WFH recommendations have a more comprehensive evidentiary approach, which includes observational studies, registry data, and expert opinion in addition to RCT results (Srivastava et al., 2020). This more general view acknowledges that in hemophilia, where therapeutic innovation and patient heterogeneity are the standard, the use of RCT data might not be sufficient to inform clinical decision-making. The evidence that can be obtained in real life, based on national registries and longitudinal cohort studies, is important information on treatment efficacy, adherence, safety, and patient-reported outcomes in long-term settings (Olivieri et al., 2025; Wheeler et al., 2025).
Real-world data is especially crucial in the assessment of newer therapies including emicizumab and extended half-life factor products. The results of observational studies and registry analyses have shown sustained bleeding rates reduction, increased adherence, and better quality of life in a wide range of patient groups, including those typically underrepresented in clinical trials (Young et al., 2024; Buckner et al., 2025). These results point to the value-added nature of real-world evidence in the ability to capture results beyond the confined setting of RCTs.
This omission of this kind of data in the development of guidelines, as observed in the ISTH framework, could thus result in an incomplete picture of therapeutic benefit. According to the critical reviews of the ISTH guidelines, the limitation to evidence to RCTs may lead to an underestimation of the effectiveness of novel treatments and inability to consider the variability in patient response and healthcare delivery settings (Kenet and Fujii, 2024; Lewandowska et al., 2025).
In addition, clinical decisions made in practice rely heavily on real-life evidence when it is impossible to achieve ideal conditions of treatment.
Observational data can be helpful in low- and middle-income countries, where access to therapies can be problematic, and the viability and efficacy of adapted treatment plans, such as low-dose prophylaxis and alternative regimens, can be assessed (Fedewa et al., 2025).
Clinical and Practical Implications of ISTH Recommendations
ISTH framework provides a narrow range of guidelines, which, though based on high-certainty evidence, might not be sufficiently representative of the challenges of hemophilia management in practice. The preference of prophylaxis treatment over episodic therapy in patients with severe or moderately severe hemophilia is one of the key recommendations of the ISTH guideline (Rezende et al., 2024). Although it is consistent with the current evidence showing lower bleeding rates and better long-term outcomes, the limitation of prophylaxis to more severe phenotypes can potentially leave the needs of patients with non-severe hemophilia with severe bleeding tendencies unaddressed (Iorio et al., 2023).
There is also an emerging body of evidence that a phenotype-based model, as opposed to adherence to baseline levels of factors, may be more suitable to inform treatment decisions.
Moreover, the ISTH guideline introduces various therapeutic modalities, such as standard half-life factor concentrates, extended half-life products, and non-factor therapies like emicizumab, which are broadly equal in the context of prophylaxis (Rezende et al., 2024). Although this is an indicator of the lack of head-to-head RCT data, it can hide clinically significant differences in the administration route, treatment burden, and patient adherence.
Indicatively, subcutaneous therapy like emicizumab has been reported in real-life studies to be significantly less burdensome to treatment and has been reported to increase adherence as compared to intravenous replacement of factors (Young et al., 2024).
The restricted status of emicizumab in specific clinical settings, especially in patients with no inhibitors, is another example of the limitations of an RCT-based methodology. Though initial studies had mainly been done on the population of inhibitors, later real-life experiences have shown significant advantages in a wider range of patients, including those who do not have inhibitors (Buckner et al., 2025). The slow integration of such evidence into the guidance recommendations can be a barrier to the prompt implementation of effective therapies in clinical practice.
The other significant implication is associated with the suggestion of plasma-derived factor VIII in particular situations, in part, because of the considerations of inhibitor development. Although this can be justified by the chosen evidence, it brings up the issue of safety, availability, and patient preference balance, especially in the environment where recombinant products are common and accepted (Chowdary et al., 2025). These recommendations can also lead to unintended effects on the development of procurement policies and clinical practice patterns. Moreover, ISTH framework enables the application of low-dose prophylaxis in resource-limited contexts, considering the differences in access to treatment globally (Rezende et al., 2024).
Global Equity and Access in Hemophilia Care
Clinical effects of the guidelines are not restricted to the treatment of the individual patients alone, but it impacts the policy of the healthcare, as well as the funding decision and the access to treatment in a universal scale. In the context of hemophilia care, where there are considerable gaps between the high-income and the low- and middle-income nations, the consequences of the guideline recommendations are especially dramatic.
Worldwide, hemophilia is not a well-diagnosed and effectively treated disease, and there is a very strong controversy regarding the differences between access to factors and concentrates of clotting factors and the best treatment.
It is approximated that as the prevalence of hemophilia is estimated to be about 800,000 people worldwide, a significant percentage of patients especially in resource-constrained environments do not have access to proper diagnosis and treatment (Fedewa et al., 2025).
The ISTH guideline, which focuses on high-certainty evidence based on RCTs, might unintentionally give preference to therapies that are highly researched in controlled settings but not necessarily available or practicable in every healthcare system (Rezende et al., 2024). Such a strategy, as advocated by the World Federation of Hemophilia, runs the risk of developing recommendations that are hard to put into practice in low-resource countries, where treatment choices often have to be made that weigh efficacy against availability and cost.
In Conversely, the WFH guidelines explicitly consider the variability of resources, providing flexible recommendations that encompass the lower-dose prophylaxis approach and alternative treatment options that suit various healthcare settings (Srivastava et al., 2020). Such flexibility is indicative of the realization that the best care is not necessarily that which is best established by the best evidence but also that which is practically feasible in a particular system. Clinical experience and real-world data thus are very important in guiding equitable care approaches.
The other significant aspect of this problem is associated with the impact of guidelines on the decisions regarding the healthcare funding and reimbursement. International guidelines are often used by policymakers and payers to decide what therapies need to be prioritized, financed, or reimbursed.
As it is mentioned in the critical reviews of the ISTH recommendations, a limited evidence base can result in the prioritization of specific treatments and restrict access to other potentially effective treatments that are not widely studied in RCTs (Lewandowska et al., 2025). This relationship can limit therapeutic decision-making and patient-centered care. Moreover, the patient advocacy activities can be undermined by the guidelines that fail to capture the reality of practice.
People with hemophilia organizations frequently use evidence that shows the superiority of newer therapies, such as quality of life and treatment burden, to push towards wider access. When this evidence is not included in the guideline recommendations, it can be harder to legitimize the use of innovative treatments, especially within limited healthcare systems (Young et al., 2024).
Criticism and Response from the Hemophilia Community
The release of the ISTH 2024 guidelines has caused much discussion in the hemophilia community, which is a wider issue of how evidence is interpreted and applied in clinical practice. Among the main criticisms, there is the fact that the guideline development process does not include real-world evidence and observational data. Although the use of RCTs strengthens internal validity, it can lead to the insufficient depiction of therapeutic efficacy, especially in the case of newer therapies that have proven significant in the everyday clinical setting (Iorio et al., 2023; Lewandowska et al., 2025).
Critics suggest that this biased approach to evidence can underrate the usefulness of innovations like emicizumab and extended half-life factor products, which have been demonstrated in real-world research to have a substantial impact and reduce treatment burden (Young et al., 2024; Buckner et al., 2025).
Moreover, there has been an outcry on the timing of the ISTH guidelines against the fast changing therapeutic environment. With the ongoing emergence of new treatments, such as gene therapy and next-generation factor products, the recommendations in the guidelines that rely on a small amount of evidence or are outdated might soon become obsolete (Samelson-Jones et al., 2024).
This problem highlights why it is difficult to keep guidelines relevant in a discipline where innovation is a constant. The possible adverse implications of the ISTH recommendations have also been pointed out with reference to healthcare policy and clinical practice. According to critical discussions and commentaries, restrictive guidelines can affect payer choices, restrict access to some therapies, and decrease the ability to be flexible when choosing a treatment (Kenet & Fujii, 2024).
To address these issues, the hemophilia community has made efforts to redefine and situate the ISTH recommendations. Interestingly, journals like the JTH in Clinic commentary have attempted to salvage the guidelines by offering more clinical background and the significance of incorporating more general types of evidence into the decision-making process.
Towards More Balanced and Inclusive Guideline Development
One of the priorities is the combination of several sources of evidence. Although RCTs are crucial in proving efficacy, they must be supported by real-life data, observational research, and registry-based evidence that reflect long-term outcomes, treatment adherence, and patient-reported experiences (Iorio et al., 2023; Wheeler et al., 2025). This is essential in hemophilia, where the rapid development of therapeutic innovations, and heterogeneous populations of patients are the order of the day, and in which case, recommendations must be relevant, and applicable.
Besides methodological inclusivity, more focus should be directed to the stakeholder engagement. The involvement of clinicians, patients, and advocacy organizations has been one of the strengths of frameworks like those created by the World Federation of Hemophilia, where guidelines are not only based on clinical evidence but also on lived experience and practical realities (Srivastava et al., 2020).
The other factor is the requirement of contextual adaptability.
Since the global differences in hemophilia care access are significant, the guidelines should be structured to support the differences in healthcare infrastructure, resource access, and access to treatment (Fedewa et al., 2025). This involves offering flexible treatment options, the importance of lower-dose strategies where needed, and not making any recommendations that can limit access to effective treatments unintentionally. As the example of the International Society on Thrombosis and Hemostasis guidelines shows, methodological choices can also affect not only clinical practice but also healthcare policy, funding priorities, and innovation in the field (Rezende et al., 2024).
Conclusion
Hemophilia care has been characterized by a fast pace of therapeutic innovation, rising clinical complexity, and a shift towards more personalized and preventive care. In this landscape, clinical guidelines are very relevant in influencing treatment decisions, standardizing care, and informing health policy. Nevertheless, as it has been seen in this analysis, such guidelines are inherently as worth as their methodologies.
The analysis of the structures of the World Federation of Hemophilia and the International Society on Thrombosis and Hemostasis shows a distinct difference in the methods. Even though the ISTH guidelines are more specifically oriented to the rigor of the methodology, occasionally with high-certainty RCT evidence, such selectivity may undermine clinical applicability, particularly in a rare, swiftly evolving disease such as hemophilia.
On the other hand, the broader and more extended approach employed by the WFH is more flexible and contextually applicable, including the real-life evidence and expert opinion and patient opinion to support the decision-making in a diverse healthcare setting. The webinar conducted by Cedric Hermans highlights the need to reconsider the process of guidelines development and implementation.
In the future, the future of hemophilia care will be determined by not only the future of therapeutic innovation but also the capacity of the clinical community to translate evidence into practice in a manner that is equitable, patient-centered, and globally relevant. To reach this objective, it will be necessary to maintain a continuous cooperation between researchers, clinicians, patients and policymakers so that the guidelines can keep up with the developments in the field of science and mirror the reality they are supposed to serve.
References
Benemei, S., Mattia, C., & Nappi, G. (2024). The good, the bad and the ugly of pain in haemophilia: Recent evidence on the epidemiology, molecular mechanisms and knowledge gaps preventing optimal treatment. Haemophilia, 30(3), 589–597. https://doi.org/10.1111/hae.15002
Buckner, T. W., Carpenter, S. L., Daoud, N., Kempton, C. L., Lee, L., Malec, L., McLean, T. W., Morton, P., O’Neill, C., Staber, J. M., Wang, M., Croteau, S. E., & Recht, M. (2025). Safety and effectiveness of emicizumab in people with haemophilia A enrolled in the ATHN 7 haemophilia natural history study. Haemophilia. Advance online publication. https://doi.org/10.1111/hae.70151
Carcao, M., & Iorio, A. (2024). How much prophylaxis is enough in haemophilia? Haemophilia, 30(Suppl. 3), 86–94. https://doi.org/10.1111/hae.14964
Chowdary, P., Carcao, M., Kenet, G., & Pipe, S. W. (2025). Haemophilia. The Lancet, 405(10480), 736–750. https://doi.org/10.1016/S0140-6736(24)02139-1
Fedewa, S. A., Valentino, L. A., Koo, A., Cafuir, L., Gillespie, T. W., Buckner, T. W., Tran, D. Q., Antun, A., & Kempton, C. L. (2025). Global patterns of hemophilia drug trials, hemophilia care, and health care measures. Research and Practice in Thrombosis and Haemostasis, 9(2), 102714. https://doi.org/10.1016/j.rpth.2025.102714
Gualtierotti, R., Solimeno, L. P., & Peyvandi, F. (2021). Hemophilic arthropathy: Current knowledge and future perspectives. Journal of Thrombosis and Haemostasis, 19(9), 2112–2121. https://doi.org/10.1111/jth.15444
Iorio, A., Königs, C., Reding, M. T., Rotellini, D., Skinner, M. W., Mancuso, M. E., & Berntorp, E. (2023). Prophylaxis use of clotting factor replacement products in people with non-severe haemophilia: A review of the literature. Haemophilia, 29(1), 33–44. https://doi.org/10.1111/hae.14676
Kenet, G., & Fujii, T. (2024). Safety of recombinant activated factor VII for treatment of breakthrough bleeds in patients with congenital haemophilia A and inhibitors receiving emicizumab prophylaxis: Review of the real-world evidence. Haemophilia, 30(2), 267–275. https://doi.org/10.1111/hae.14933
Lewandowska, M., Nasr, S., & Shapiro, A. D. (2025). Emerging therapies in hemophilia: Improving equitable access to care. Journal of Blood Medicine, 16, 95–115. https://doi.org/10.2147/JBM.S490588
Olivieri, M., Yan, S., Yang, Y., Tomic, R., Linhoff, T., Zhang, X., Drelich, D., Jakobs, N., & Miesbach, W. (2025). Comparing real-world outcomes of prophylaxis with extended half-life factor IX (rIX-FP vs. rFIXFc and N9-GP) for haemophilia B: An analysis of medical chart data from Germany. Advances in Therapy, 42(11), 5696–5707. https://doi.org/10.1007/s12325-025-03336-y
Pfrepper, C., Ettingshausen, C. E., Klamroth, R., Oldenburg, J., & Olivieri, M. (2024). Expert opinion for defining a severe bleeding phenotype to guide prophylaxis in patients with nonsevere hemophilia. Hamostaseologie. Advance online publication. https://doi.org/10.1055/a-2411-7416
Rezende, S. M., Neumann, I., Angchaisuksiri, P., Awodu, O., Boban, A., Cuker, A., Curtin, J. A., Fijnvandraat, K., Gouw, S. C., Gualtierotti, R., Makris, M., Nahuelhual, P., O’Connell, N., Saxena, R., Shima, M., Wu, R., & Rosendaal, F. R. (2024). International Society on Thrombosis and Haemostasis clinical practice guideline for treatment of congenital hemophilia A and B based on the GRADE methodology. Journal of Thrombosis and Haemostasis. Advance online publication. https://doi.org/10.1016/j.jtha.2024.05.026
Rodeghiero, F., Ghiotto, L., Pontalto, L., Casini, A., Castaman, G., Abdul-Kadir, R., Berntorp, E., Bodó, I., Degenaar-Dujardin, M., Fijnvandraat, K., Gresele, P., Key, N. S., Lassila, R., Lillicrap, D., Makris, M., Meijer, S., Mezzano, D., Noris, P., & Pabinger, I. (2025). Mild or moderate hemophilia is not always a mild or moderate bleeding disorder: Back to the clinical phenotype. HemaSphere, 9(3). https://doi.org/10.1002/hem3.70111
Samelson-Jones, B. J., Small, J. C., & George, L. A. (2024). Roctavian gene therapy for hemophilia A. Blood Advances, 8(19), 5067–5076. https://doi.org/10.1182/bloodadvances.2023011847
Srivastava, A., Santagostino, E., Dougall, A., Kitchen, S., Sutherland, M., Pipe, S. W., Carcao, M., Mahlangu, J., Ragni, M. V., Windyga, J., Llinás, A., Goddard, N. J., Mohan, R., Poonnoose, P. M., Feldman, B. M., Lewis, S. Z., Berg, H. M., & Pierce, G. F. (2020). WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia, 26(Suppl. 6), 1–158. https://doi.org/10.1111/hae.14046
Wheeler, A. P., Abraham, A., Barnes, C., Brown Frandsen, R., d’Oiron, R., Eichler, H., Hampton, K., López-Jaime, F. J., Lyu, C. J., Tavares, C. M. M., Nogami, K., Sutton, C., Windyga, J., Zulfikar, B., & Castaman, G. (2025). Real-world unmet needs of patients with haemophilia A and haemophilia B with or without inhibitors: End-of-study results from the explorer6 non-interventional study. Haemophilia, 31(5), 903–911. https://doi.org/10.1111/hae.70051
Young, G., Pipe, S. W., Kenet, G., Oldenburg, J., Safavi, M., Czirok, T., Nissen, F., & Mahlangu, J. (2024). Emicizumab is well tolerated and effective in people with congenital hemophilia A regardless of age, severity of disease, or inhibitor status: A scoping review. Research and Practice in Thrombosis and Haemostasis, 8(4), 102415. https://doi.org/10.1016/j.rpth.2024.102415